Male Factor Infertility.
Its interesting, over the last number of years while working with couples trying to have a baby, some unusual patterns have developed in my clinic. Todays writing piece is going to be about the ‘XY’ Chromosomes of this planet, we call earth. These species are called ‘Men’ You will see them roaming the earth, some being tall, others small, young and old, balding and hairy. For some of those men, I have to say, I am so proud to call myself a ‘Man’ as I stand shoulder to shoulder with them, in the way I see them support their partners during their fertility journey in unity, with purpose. And then, there are the others, where I just want to get a wet fish and slap them across the head. What I find amazing its amazing there doesn’t seem to be a middle ground, men are either ‘Super Men’ or just ‘Stupid Jerks’ and wow, they can be Jerks.
It is now know in the medical community that over 40% of all issues related to infertility are male related, yes I will say that again, and again and again, 40% of all infertility with couples trying for a baby is down to men. So if you have been trying for a baby for a while now, and it seems to be unexplained and your partner has not been checked out. Send him for a sperm analysis today.
So first off, lets get some of the Science out of the way:
Men start to produce male sex hormones at puberty, usually between 11 and 14 years of age, where the Pituitary gland secretes FSH and LH hormones which stimulate the testicles to produce sperm. The LH hormone also stimulates the testis to produce testosterone inn the male. This inturn promotes the development of the man such as facial hair, deeper voice and other male characteristics.
With the male anatomy we have the penis and scrotum and within the scrotum are two testis. The sperm are stored here and are connected to the vas deferens, a tube like structure which is then connected to an ejaculatory duct, which joins to the urethra, a tube that passes inside the penis. Sperm takes between 75 and 90 days to develop from start to finish, and cells divide over 360 times. Once the sperm is fully formed and ready for ejaculation, they are propelled into the urethra where they mix with secretions from the prostate. Sperm holds about 15-25% of this mix, and there are about 25 different chemical like substances that support the growth and development of the sperm. After ejaculation, this fluid is very viscus, but will however liquify afer 10 to 15 minutes, so the sperm can travel through the cervix and be supported by the cervical secretions. Travelling to the egg for fertilisation.
In my clinic I would say that only 1 in 10 men have ever come into me, where 50% of them are coming to make sure Im not some cracked snake oil peddler making promises I definitely would never make. They usually come in with a very stern look and ready to take me on. It actually sometimes feels like Im in the wild west and we are standing in front of each other ready to draw our guns, watching every move of the guy in front of each other. Usually after the 1st session I never see them again. The other type, is usually very quite in the 1st session, and waits in reception with his partner and never looks at me. Says about two words during the initial consult. But is like an eagle, watching everything from above, listening intensely, taking everything around them. These guys I like. They are committed to the process, they’re not sure at first, but once they are in, they are like ‘Fertility Triathletes ‘ They will do what ever it takes to get to the end.
In men, infertility is defined as the inability to fertilize the an egg, whereas sterility is defined as the lack of sperm production. Male fertility depends upon three things:
(1) adequate production of spermatozoa by the testicles,
(2) unobstructed transit of sperm through the seminal tract, and
(3) satisfactory delivery to the egg.
The analysis of sperm count, motility and morphology are the main parameters which gauge a man’s ability to support conception. There are other factors that are also important such, the quality of the seminal fluid, liquefaction, and the ability for the sperm to be inserted into the vagina where fertilisation can occur.
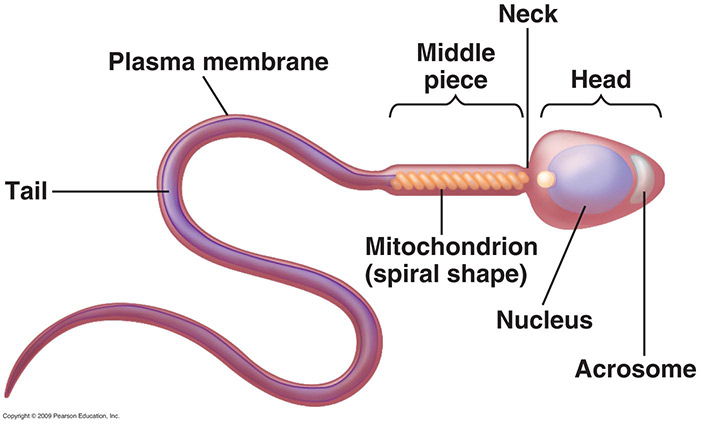
So what does a good looking sperm look like, well it need to be like the picture below. Where there is a good head, body and tail. Formation is key to the success of fertilisation. In alot of cases the sperm will not look like the sperm below. Sometime there may be only 2-3% of the sperm correctly formed.
Some of the Sperm evaluations:
– adequate
– aspermia (absence of ejaculate by the male)
– azoospermia (absence of sperm in semen)
– oligospermia (lowered sperm density in the analysis)
– poor motility (impaired forward movement by the sperm)
– morphology (high percent of abnormal sperm which won’t fertilise an egg)
– antisperm antibodies (which has been affected the the immune system)
Most infertility evaluations for men include an analysis of a man’s semen. Where there can be:
– deficient sperm count (less than 15 million per milliliter; volume should be 1 to 5 milliliters of ejaculate)
– insufficient sperm motility (over 50 percent should be motile and demonstrate purposeful forward movement), and/or
– poor sperm morphology (more than 5% Kruger analysis)
In 35 to 40 percent of cases of infertility, sperm abnormalities are a major factor in the couples inability to conceive a baby. However, men are usually that last port of call when a couple is trying for a baby, and it can be more than two years before the man is tested. This to me is something that needs to be seriously addressed so that a couple don’t waste a massive amour of time trying to find out later that the male factor was the cause of the infertility.
On average, a male ejaculate will contain over 200 million sperm, by the time the sperm has completed its journey, there may be only 2 dozen sperm left to fertilise the egg, so statistically when you hear it only takes one sperm, that is a very unfair assessment to the situation.
The average ejaculate sample contains almost 200 million sperm, however only a few dozen sperm actually reach the egg for a chance at penetration. This makes for some pretty ominous statistics for sperm overall. Sperm numbers must be high just to have a modicum of hope of reaching the vicinity of the egg that is traveling down the fallopian tube. Its interesting to note through the WHO (World Health Organisation) that sperm counts have dropped by over 50% in the last 40 years. To which I would argue defines an issue of epidemic pre portions. Sperm are just as susceptible as eggs to environmental influences, such as toxins, environmental issues, poor diet, infections and both prescription and non prescription drugs. Something as simple as an antihistamines can negatively affect sperm count by diminishing the quantity of seminal fluid. Stress, lack of sleep, and overuse of alcohol, nicotine, and marijuana decrease sperm production quality. It takes approximately three months for sperm to develop fully. When a result is poor, the standard call by the medical community is it can’t be fixed. Or there is no diagnosis as to why it is an issue.
So if a result is poor there are a number of areas that need to be looked at:
– Count: the current minimum count for a man to be defined as fertile is 15million. It’s important to remember that this is a minimum, anything below this number makes the man technical infertile. So if you look at it that 15 to 20 million is the equivalent of getting a ‘D’ in his exams. 20 to 35 million would be a ‘C’ etc etc. The unfortunate thing is that a man can have results give to him and they might be borderline, maybe 15.5 million and he is give the all clear technically. However it’s so important to look at the rest of the picture.
– Morphology: As important are the lab result for mortality and morphology. Mortality is bacally the speed and direction of the sperm, are they moving rapid ally or slowly and are they going in the right direction. The morphology in my opinion is the most important fact of all, currently the WHO recommend that the morphology be at 4%, which means that 96% of sperm will not fertilise an egg. Have a think about that. 96% of his sperm under analysis won’t fertilise an egg…
– Antisperm antibodies: Other areas that are being evaluated more frequently are antis perm antibodies, they can be produced by either partner, they perceive the sperm as being dangerous and attack the sperm, killing them off before they reach the egg. The best solution for men with antis perm antibodies is to go to a fertility clinic where the sperm can be washed in a special solution that removes the antibodies.
Sperm works inn conjunction with spinal fluid, this is by nature alkaline in nature, for women the cervix and vaginal fluids tend to be more acidic except around ovulation time when the become more alkaline due to the cervical secretion changes. The secretions make the cervix more sperm friend, and contain proteins and nutrients to support development and growth of the sperm as soon as i separates from the seminal fluid.
Seminal fluid is very alkaline; the vaginal environment and cervical secretions are very acidic, except around ovulation when the vaginal secretions become more alkaline for sperm survival. Interestingly, male (Y) sperm have a greater ability to survive in acidic cervical mucus. Male sperm are also faster than female (X) sperm; female sperm can survive longer inside the female reproductive organs than male sperm.
In Western Medical terms there is very little that can be done to improve male factor infertility, however some success have been seen with certain diet and lifestyle changes. The next few paragraphs are going to get very technical so you can skip to the end now if you wish.
So how does it all work, well, Dr Lewis, of The Fertile Soul explains it as follows: the seminal vesicles secrete substances including fructose which feeds the sperm, fibrinogen which holds the fluid together, and prostaglandins which help the sperm penetrate the cervix. The prostate adds an alkaline fluid to the ejaculate. Seminal fluid in normal, fertile men contains antioxidant factors. In many sub-fertile men the seminal fluid may not contain these protective elements, or the circulating free radicals may be so abundant that the seminal fluid is not capable of eliminating the damaged cells. Therefore, men with sub-optimum sperm counts should include dietary sources of antioxidants like wheat and barley grass, sprouts, and dark green vegetables.
Also, the plasma membrane of human sperm contains high levels of polyunsaturated fatty acids, making them extremely susceptible to damage by free radicals, which can lead to lower motility and morphology, so adding unsaturated fatty acids like those found in sesame, almond, flax seed, hazelnut, pecan, pumpkin seed, sunflower seed, pine nut, walnut, olive, avocado, soybean, and quinoa, and omega-3 fatty acids found in fish oil to the diet can help sperm integrity.
Many environmental and dietary factors are hostile to the production of healthy sperm. For example, estrogen is important in sperm formation, but consuming too much synthetic estrogen in the diet can be harmful. Unfortunately, most meat, dairy products, and even poultry and eggs contain substantial quantities of synthetic estrogens. Some reports have shown the presence of synthetic estrogen in sources of drinking water as well. Therefore, eating only hormone-free meat, poultry, eggs, and dairy products, and drinking only purified drinking water is suggested. Many environmental toxins such as pesticides and other chemicals found in non-organically grown produce also can impair spermatogenesis, so you should consume only organic fruits and vegetables whenever possible. To support cardiovascular and reproductive health, avoid saturated fats, hydrogenated oils, coconut, palm, and especially cottonseed oil (it contains gossypol, a chemical that inhibits sperm formation). Include polyunsaturated oils and essential fatty acids: both these contribute to the health of the sperm and seminal fluid.
Oxidative damage is present in almost half of the diagnosed cases of insufficient sperm count. The seminal fluid contains high levels of antioxidants, but when the development of healthy sperm becomes impaired because of environmental toxins, stress, or pharmaceutical agents, the seminal fluid will be found to have elevated levels of oxidants.
Free radicals (which float around the body and damage other cells) are said to be responsible for 40 percent of sperm damage can be overcome with antioxidants found in blackberries, blueberries, garlic, kale, strawberries, brussels sprouts, plums, alfalfa sprouts, broccoli, and red peppers.
If the seminal fluid is too viscous, the sperm cannot travel freely through the cervix.
Another potential problem with sperm viability is incompatibility with a woman’s cervical mucus. It is extremely important to keep the sperm in a more alkaline environment because the vaginal pH is relatively acidic. If a woman’s cervical and vaginal environment is too acidic, the sperm will not be able to survive.
Im still amazed every day at how all this works and sometimes doesnt.
So what options do we have, well we can look at creating a ‘Super Sperm Diet’, when I worked in the US with Dr Lewsi, this would be a stand rd approach we would take to treating men.
The following are a list of those foods that can enhance sperm production.
Amino Acids – The building blocks of life. Necessary for egg and sperm production.
Vitamin A – Essential for the production of male sex hormones.
A deficiency is shown to reduce sperm volume and count, and increase abnormal sperm.
Vitamin B6 – Together with zinc, B6 is essential for the formation of male sex hormones.
Vitamin B12 – Folate and B12 are needed for the synthesis of DNA and RNA. These make up the blueprint for the genetic code of the entire body. Low levels can cause abnormal sperm production, reduced sperm counts, and reduced motility. even if your count is only on the low side, supplement with B12.
Folic acid – Needed for sperm production, count, motility, and low morphological abnormalities.
Vitamin C – An antioxidant that prevents damage from free radicals. It is needed for the healthy production of sperm. Low vitamin C levels have been linked with an increase in birth defects. It can increase count and motility of sperm. It is also shown to reduce clumping of sperm.
Vitamin E- Diets lacking in the antioxidant vitamin E do not support the reproductive function. Vitamin E may also help the sperm penetrate the egg.
Zinc – Deficiencies of Zinc are quite common. Zinc is important for the cell division and the production of healthy sperm. It is the most critical trace mineral for male sexual function. It is needed for testosterone metabolism, testicle growth, sperm production, motility, count, reducing excess estrogen in male reproductive tissue.
Coenzyme Q10 – Important for energy production. Fertilization rates may rise when taking this supplement. It also improves blood flow. It is present in large amounts in the seminal fluid. It protects them against free radical damage, gives sperm energy (along with fructose), and increases their motility.
On a final note, something you may not have know, is that it is the male sperm that determines the sex of the baby. You will have heard of X and Y chromosomes The mothers egg always carries the female chromosome which is given the X label, where as the father carries either the X, female or Y, the male chromosome. So depending on whether you get an XX or XY, will determine the sex of the child. Isnt the beautiful of nature just amazing.
This is definitely the fins; note, lots of couples ask me what are the chance of improving the quality of sperm, and to be honest for some men, its works amazingly well, and we would see massive improvements in the men on the program over 3 – 4 months. However, in 30-40% of the cases there is no change, and I think this comes down to male hormone insufficiency.
OK, I LIED, last thing. I Promise. When you or your partner gets a poor result from their semen analysis and you ask the question, how did this happen, and what can we do to fix it. Don’t ask a Gynaecologist this question, they have trained in female anatomy, and will have a basic understanding of male fertility. Look for a specialist in Andrology who has a background in Urology. And also understands male fertility.
Asking your Gynaecologist for advice on sperm is like having your local car mechanic looking at the engine of a Boeing 747, thats one plane I would NOT be flying on if that happened.. Take care, Gordon.